Direct Anterior Approach: Muscle Sparing Hip Replacement Surgery
By Dr. Cory Calendine, MD | Board-Certified Orthopedic Surgeon | Bone and Joint Institute of Tennessee
Last updated: March 2026
TLDR: Muscle sparing hip replacement surgery uses the direct anterior approach to access your hip joint through natural gaps between muscles instead of cutting through them. This means less tissue damage during the procedure, which typically leads to less pain after surgery, a faster return to walking, and a quicker overall recovery. Most patients are walking within hours and heading home the same day or the next morning.
What Makes a Hip Replacement "Muscle Sparing"?
Your hip can be reached from several directions during replacement surgery. The traditional posterior approach goes through the back of the hip, and the lateral approach enters from the side. Both of these routes require cutting through muscles and tendons to reach the joint. Those tissues then need to heal after surgery, which adds time and discomfort to your recovery.
The direct anterior approach takes a different path. It enters through the front of the hip, using a natural interval between two muscles: the tensor fascia lata and the sartorius. Instead of cutting through muscle fibers, the surgeon gently separates these muscles and works between them. Once the procedure is done, the muscles are moved back into their normal position.
Think of it this way. If you need to reach something in a packed closet, you could tear the door off the hinges and rebuild it later. Or you could simply open the door, get what you need, and close it. The muscle sparing approach is like opening the door. The structures that were there before the surgery remain intact afterward.
This concept matters because the muscles you don't cut are muscles you don't have to rehabilitate. That single difference drives many of the recovery advantages patients experience with this technique.
Why Does the Surgical Approach Matter for Your Recovery?
The way your surgeon accesses your hip joint has a direct impact on how you feel in the days and weeks after surgery. When muscles are cut and then repaired, your body has to heal those tissues on top of recovering from the joint replacement itself. That means more pain, more inflammation, and more time before you feel like yourself again.
With muscle sparing hip replacement, the soft tissue trauma is significantly reduced. In my practice, I see patients walking within hours of their procedure. Many go home the same day. Some patients have told me that the surgical pain was actually less than the arthritis pain they had been living with before the operation. That tells you something about how much tissue preservation matters.
Research supports these clinical observations. A randomized study from the Mayo Clinic compared the direct anterior approach to the mini-posterior approach and found that anterior patients stopped using a walker at 10 days compared to 14.5 days for the posterior group. They also discontinued all walking aids at 17 days versus nearly 24 days, and they stopped taking narcotic pain medication at about 9 days compared to 14 days.
The early recovery differences are real and meaningful for patients who want to get back to their daily routines.
How Is Muscle Sparing Hip Replacement Performed?
During a muscle sparing hip replacement using the direct anterior approach, you lie face up on a specialized surgical table. This supine position is actually one of the key technical advantages. Because your pelvis stays level, the surgeon can use live fluoroscopy (real-time X-ray imaging) throughout the entire procedure.
That live imaging works like GPS in the operating room. It allows your surgeon to check implant positioning, leg length, and component alignment while the surgery is still in progress. If anything needs adjustment, it can be corrected right then before closing.
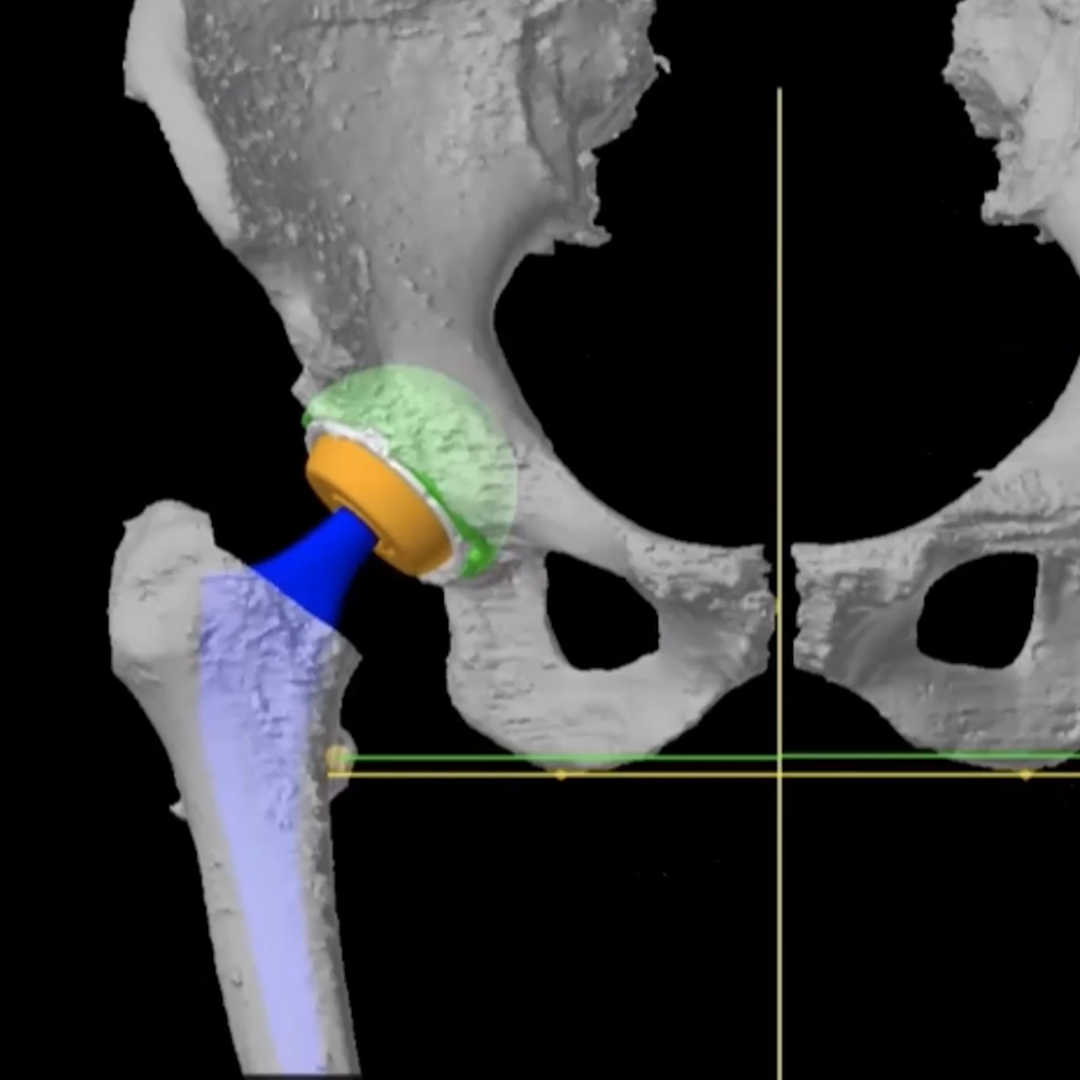
The incision is typically three to four inches long, placed near the front of the hip. After the surgeon separates the muscles and opens the hip capsule, the worn-out femoral head (the ball of the joint) is removed. The acetabulum (the socket) is prepared and fitted with a titanium shell and a polyethylene liner. On the femur side, the bone canal is shaped to accept a titanium stem, and a new ceramic or metal ball is placed on top. The hip is then reduced, meaning the new ball is seated into the new socket.
Before closing, a final X-ray confirms that leg length is equal, alignment is correct, and every component is positioned where it should be. The wound is closed in layers, and the muscles settle back into their natural positions without requiring reattachment.
What Does Recovery Look Like After Muscle Sparing Hip Replacement?
Recovery after muscle sparing hip replacement tends to move faster than most patients expect. Here is a general timeline based on what I see in my practice at the Bone and Joint Institute of Tennessee:
Day of surgery: Most patients are up and walking with the help of a physical therapist within a few hours of their procedure. Many go home the same day or the following morning.
First two to three weeks: You will likely use a cane or walker during this period. Pain is typically well-managed with over-the-counter medications, and many patients reduce or stop narcotic pain medication within the first week to 10 days.
Two to four weeks: Most patients are driving and handling basic daily activities. The cane is usually no longer needed by the end of this period.
Six weeks to three months: Gradual return to more demanding activities, recreational sports, and exercise programs. By the three-month mark, most patients are functioning at a high level.
One of the other advantages of the muscle sparing approach is that many surgeons, myself included, do not place the same strict hip precautions that are common after posterior hip replacement. Traditional restrictions like avoiding crossing your legs, not bending past 90 degrees, and staying out of low chairs for six weeks are often unnecessary with the anterior approach. You move to your comfort level from day one.
Is Muscle Sparing Hip Replacement Right for Everyone?
I want to be straightforward about this. While the muscle sparing anterior approach works well for the majority of patients, it is not the ideal choice in every situation.
Patients with certain body types, including those who are very muscular or who carry significant weight in the midsection, can present a more challenging exposure through the front of the hip. Patients with prior hip hardware on the back side of the joint or those with specific acetabular deficiencies may be better served by a posterior approach that provides direct access to those areas.
There is also a well-documented learning curve for surgeons adopting this technique. Research shows that complication rates drop significantly after the first 50 to 100 cases. Surgeon experience with the approach plays a major role in outcomes. That is why choosing a surgeon who regularly performs this procedure is one of the most important decisions you can make.
The research also shows something worth understanding about long-term results. While the anterior approach consistently demonstrates advantages in early recovery, including less pain, faster mobilization, and quicker return to function, by three to six months the functional outcomes between approaches tend to equalize. Both the anterior and posterior approaches produce excellent long-term results.
So the goal is never about declaring one approach better than another across the board. It is about matching the right approach to the right patient with the right surgeon.
What Are the Risks of Muscle Sparing Hip Replacement?
Like any surgical procedure, muscle sparing hip replacement carries some risks. Understanding these helps you make an informed decision.
Lateral femoral cutaneous nerve irritation is the most commonly discussed risk specific to the anterior approach. This nerve runs near the incision and can become stretched during surgery, leading to numbness or tingling along the outer thigh. In most cases, this resolves within a few months.
Femoral fractures can occur, particularly during the learning curve period for surgeons new to the approach. This risk decreases significantly with surgeon experience and proper technique.
Dislocation rates are generally lower with the anterior approach compared to the posterior approach. The preserved muscles act as natural stabilizers for the new joint. Studies of over 1,000 anterior hip replacements have confirmed this lower dislocation risk.
Wound complications can be slightly more common with the anterior approach, especially in patients with higher body mass index. The incision location near the groin crease can be affected by skin folds in larger patients.
Infection rates are similar across all surgical approaches and remain low overall for hip replacement surgery.
When Should You Talk to a Surgeon About Hip Replacement?
If hip pain is limiting your ability to walk, sleep, climb stairs, or enjoy the activities that matter to you, it may be time to have a conversation with an orthopedic surgeon. Most patients who reach the point of considering hip replacement have already tried conservative treatments like physical therapy, anti-inflammatory medications, and injections without lasting relief.
You don't need to wait until you can barely move. In fact, patients who are still reasonably active tend to recover faster because they have better muscle strength going into the procedure.
Here are some signs that it may be time to schedule an evaluation:
- Pain that wakes you up at night or prevents restful sleep
- Difficulty putting on shoes or socks due to hip stiffness
- Needing to limit walking distances because of hip discomfort
- Relying on anti-inflammatory medications daily just to get through normal activities
- Hip pain that has not improved with physical therapy or injections
Muscle Sparing Hip Replacement in Franklin and Nashville, Tennessee
Hip replacement remains one of the most successful operations in all of medicine. It reliably eliminates pain, restores function, and gives people their quality of life back. The muscle sparing direct anterior approach has made an already successful surgery even better for many patients, particularly during those critical first weeks of recovery.
If you are dealing with hip pain and want to learn whether muscle sparing hip replacement is right for you, I see patients at the Bone and Joint Institute of Tennessee in Franklin, serving Brentwood, Nashville, and the greater Middle Tennessee area.
Medical Disclaimer: This information is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Surgical procedures carry risks and benefits that vary for each individual. Always consult with a qualified orthopedic surgeon to discuss your specific situation, risks, and expected outcomes.
Ready to Take the Next Step?
If hip arthritis is affecting your quality of life, schedule a consultation to discuss your treatment options. Dr. Cory Calendine is a board-certified orthopedic surgeon specializing in hip and knee replacement at the Bone and Joint Institute of Tennessee in Franklin, TN.
About the Author
Dr. Cory Calendine is a board-certified orthopedic surgeon specializing in joint replacement of the hip, knee, and shoulder. He practices at the Bone and Joint Institute of Tennessee, part of Williamson Health, located in Franklin, Tennessee. Dr. Calendine is dedicated to providing personalized, evidence-based orthopedic care to patients throughout Middle Tennessee.
Frequently Asked Questions
How long does muscle sparing hip replacement surgery take?
The procedure typically takes about 60 to 90 minutes, depending on the complexity of the case. Because the approach works between muscles rather than through them, experienced surgeons can perform the surgery efficiently without sacrificing precision or safety.
Can you walk the same day after muscle sparing hip replacement?
Yes. Most patients who undergo muscle sparing hip replacement through the direct anterior approach are walking with a physical therapist within a few hours of surgery. Many patients go home the same day or the following morning.
What is the difference between muscle sparing and traditional hip replacement?
The main difference is how the surgeon reaches the hip joint. Traditional approaches typically require cutting through muscles and tendons, which then need time to heal. The muscle sparing direct anterior approach works through a natural gap between muscles, preserving the surrounding soft tissues and allowing for a faster early recovery.
How long before I can drive after muscle sparing hip replacement?
Most patients return to driving within two to three weeks after surgery, depending on which hip was replaced and whether you drive an automatic or manual transmission. Your surgeon will provide guidance based on your individual progress.
Does muscle sparing hip replacement have fewer restrictions after surgery?
Many surgeons who use the direct anterior approach do not place the same strict hip precautions that are standard after posterior hip replacement. Restrictions like avoiding crossing your legs or not bending past 90 degrees are often unnecessary because the muscles that stabilize the hip were not disrupted during surgery. You typically move to your comfort level from day one.
References:
- Galakatos GR. Direct Anterior Total Hip Arthroplasty. Missouri Medicine. 2018;115(6):537-541.
- Kyriakopoulos G, Poultsides L, Christofilopoulos P. Total hip arthroplasty through an anterior approach: the pros and cons. EFORT Open Reviews. 2018;3:574-583.
- Taunton MJ. Direct Anterior Hip Arthroplasty. Mayo Clin Surg Update. 2017;11(2):2-3.
- Barrett WP, Turner SE, Leopold JP. Prospective Randomized Study of Direct Anterior vs Postero-lateral Approach for Total Hip Arthroplasty. J Arthroplasty. 2013;28:1634-1638.
- Higgins BT, Barlow DR, Heagerty NE, Lin TJ. Anterior vs. posterior approach for total hip arthroplasty, a systematic review and meta-analysis. J Arthroplasty. 2015;30:419-434.

%20Resurfacing%2C%20CORY%20CALENDINE%2C%20MD.png)